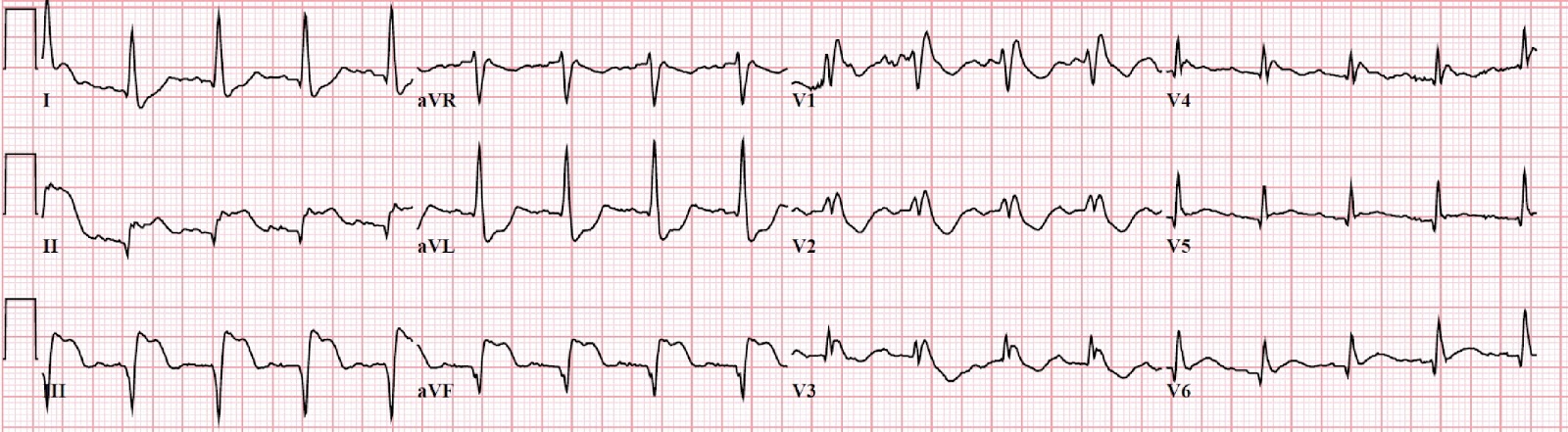
Not a mystery - this is an inferior STEMI, resulting from a total occlusion of the mid-RCA. And it looks like a nasty one. First of all, the infarct apparently covers a good deal of myocardium, since we see:
- Marked elevation in leads II, III and aVF (inferior wall)
- Subtle ST elevations in V5 and V6 (lateral wall)
- ST depression in leads V2 and V3 out of proportion for a RBBB ("posterior" wall)
What's the medical term for "tombstone elevations?"
Besides having an ominously picturesque name, does the morphology of the STEMI here contain prognostic information? Actually, this phenomenon has been well studied.
"Tombstone" ST segment elevation is more accurately described as a STEMI with either "grade 3 ischemia" or "terminal QRS distortion (TQRSD)." It's defined in the inferior leads as a J point that is higher than half-way up the R wave.
 | ||
| Examples a-d do not show TQRSD, examples e-f do show TQRSD. |
It turns out that (on average) a STEMI with TQRSD has a significantly worse prognosis than those without TQRSD. More troponin release, bigger infarcts, poorer response to reperfusion therapy, and worse in-hospital mortality.
After seeing the ECG, the ED team performed a focused echo, expecting to find significant systolic dysfunction.
So how terrible was the ejection fraction?
Actually.... not too bad. Pretty good, in fact.
Sometimes our patients don't read the textbooks, and their hearts don't keep up with the electrocardiography literature!
The post-PCI formal echo did not reveal any significant wall motion abnormalities. Aside from a bout of VF during stent placement, the patient did great!
Open-access references:
Prognostic significance of the admission electrocardiogram in acute myocardial infarction.
Prognostic significance of the distortion of terminal portion of QRS complex on admission electrocardiogram in ST segment elevation myocardial infarction.